
A Lake, Smit & Partners first: Microwave ablation for ilioinguinal nerve entrapment following multiple groin hernia repairs
Inguinal neuralgia post hernia repair is characterized as a burning or throbbing pain referred to the groin or medial thigh.
This can result from entrapment of the ilioinguinal, genitofemoral or iliohypogastric nerves post inguinal hernia repair.
The pain from the chronic inguinal neuralgia can be debilitating. The ilioinguinal nerve is the dominant nerve responsible for inguinal neuralgia.
Inguinal neuralgia can be challenging to treat with indifferent results from pain medication, behavioural therapy, nerve blocks and repeated surgery.
Various other techniques including cryoablation, radiofrequency ablation, removal of hernia repair mesh and surgical neurectomy and chemical ablation with alcohol and phenol have been used with variable results.
Most of the above have poor long term outcomes.
Microwave ablation has been demonstrated to be an alternative to radiofrequency ablation in the treatment of tumours of the chest and abdomen.
The objective of Microwave ablation is to heat the target site to create cellular necrosis. Several studies have shown an 80 -85% resolution of the inguinal neuralgia at 12 months follow up.
At Lake, Smit & Partners, our body interventional team, lead by Dr Gareth Bydawell has considerable expertise and experience in use of MV ablation with tumours of the chest and abdomen.
In a detailed discussion with the patient, an MV ablation was offered to the patient.
This was a first for Lake, Smit & Partners interventional and MSK team.
Patient:
An elderly patient had a history of recurrent hernia repairs and had suffered intractable left inguinal pain for two years.
Ten days prior to the procedure, the patient underwent a successful perineural block of his entrapped left ilioinguinal nerve with complete pain relief of 36 hrs duration.
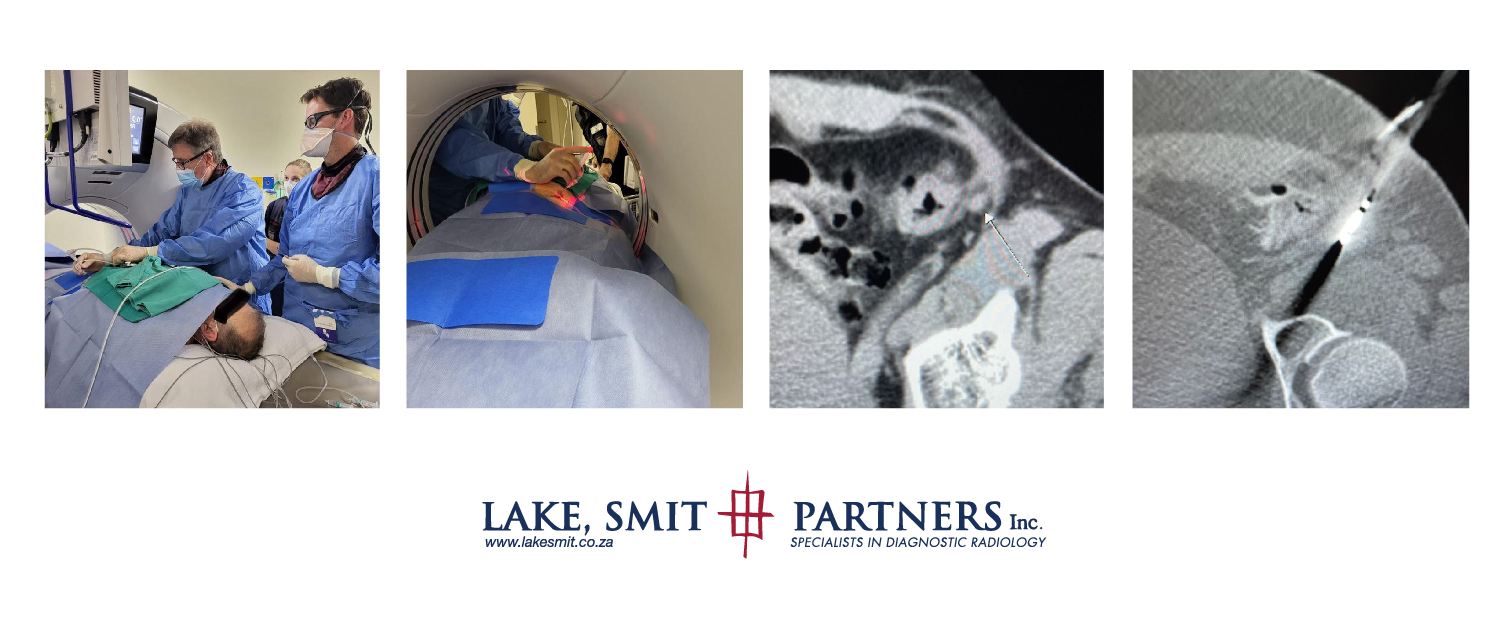
The microwave ablation was performed with CT guidance under conscious sedation with an anaesthetist in attendance. Procedure performed together by LSP radiologists Dr Gareth Bydawell and Dr John Zietkiewicz.
The nerve was ablated with 3 x 20-sec microwave ablations spaced by a two-minute gap.
Initial follow-up with the patient is encouraging.
His comment :
“Thanks Docs, Everything OK at this moment.Appreciate your help after 2 years of going through HELL”